Online Blended Bimonthly Assignment MAY 2021 Roll no. 16
Medicine Bimonthly Assignment MAY 2021
Roll No. 16 ;Ch Savanth Reddy (2k17)
1) Pulmonology
A)
https://soumyanadella128eloggm.blogspot.com/2021/05/a-55-year-old-female-with-shortness-of.html
1Q) What is the evolution of the symptomatology in this patient interms of an event timeline and where is the anatomical localisation for the problem and what is the primary etiology of the patient problem ?
1Ans)Evolution of symptomatology
1st episode of sob - 20 yr back
2nd episode of sob - 12 yr back
From then she has been having yearly episodes for the past 12 yrs
Diagnosed with diabetis - 8yrs back
Anemia and took iron injections - 5yr ago
Generalised weakness - 1 month back
Diagnosed with hypertension - 20 days back
HRCT showed Signs of - 20 days ago
Bronchiectasis
Pedal edema - 15 days back
Facial puffiness- 15 yrs back
Anatomical location of problem - lungs
Primary etiology of patient- usage of chulha since 20 yrs might be due to chronic usage
2Q)What Are mechanism of action indication and efficacy over placebo of each of the phramacological and nonphramacological interventions used for this patient?
1)Head end elevation :
.improves oxygenation
.decreases incidence VAP
.decreases incidence of aspiration
#Indication:
head injury
.meningitis
.pneumonia
Efficacy of head of bed elevation :
Significant increases in end-expiratory lung volume were seen at both 20° and 30° HOBE in all lung regions, except the anterior, with the largest changes from baseline (supine) seen at 30°. From baseline to 30° HOBE, global EELI increased by 1,327 impedance units (95% CI 1,080-1,573, P < .001). EELI increased by 1,007 units (95% CI 880-1,134, P < .001) in the left lung region and by 320 impedance units (95% CI 188-451, P < .001) in the right lung. Posterior increases of 1,544 impedance units (95% CI 1,405-1,682, P < .001) were also seen. EELI decreased anteriorly, with the largest decreases occurring at 30° (-335 impedance units, 95% CI -486 to -183, P < .001)
Conclusion :
HOBE significantly increases global and regional end-expiratory lung volume; therefore, unless contraindicated, all mechanically ventilated patients should be positioned with HOBE
2)Oxygen inhalation to maintain spo2
3)Bipap:
Assist ventilation by delivering positive expiratory and inspiratory pressure with out need for Endotracheal intubation.
Efficacy of Bipap Over Placebo :
The 10 patients in the active NPPV group rapidly improved and none needed intubation. Placebo NPPV resulted in no change in the clinical condition of patients that continued to worsen and the 10 patients were crossed over to active NPPV. Three patients were intubated. No differences in terms of morbidity, length of stay or mortality between the two groups were observed. Active NPPV (but not placebo NPPV) led to a rapid and significant improvement in the clinical parameters, pH and the carbon dioxide tension in arterial blood and to a decrease in respiratory frequency and sternocleidomastoid EMG activity.
3Q. Cause for current acute excerbation -
Infection Exacerbates COPD.
4Q.Could the ATT affected her symptoms ? if so how ?
Patient developed Edema and Facial Puffiness few days after the Initiation of ATT.As we all Know Isoniazid and Rifampicin are Hepatotoxic may be it resulted in these Symptoms.

5)What could be the Cause of Electrolyte Imbalance ??
Patients with acute exacerbation of COPD present not only with the features of acute respiratory infections (productive cough, dyspnea etc) but also a number of metabolic disorders like hyponatremia, hypokalemia, hypomagnesemia, hyperbilirubinemia, elevated transaminases, elevated blood urea and elevated serum creatinine arising out of the disease process or as a consequence of the therapy (such as beta2 agonists, steroids, diuretics etc). Very often they are missed or confuse the diagnosis, thus simple overlooking of the coexisting metabolic abnormalities may contribute to a great deal of mortality and morbidity in the COPD patients.8 Water retention and hyponatremia are typically observed in the nal stages of COPD and the onset of edema is a poor prognostic factor. In these patients the gas exchange impairment induces several hormonal abnormalities: renin (Rn), angiotensin II (AnII), aldosterone (Ald), atrial natriuretic peptide (ANP), vasopressin (ADH) and endothelial factors are some of the factors involved. The systemic response to hypercapnia has the effect of reducing the renal blood ow and, as a result, increasing water and sodium retention with the final effect of edema and hyponatremia.
https://kausalyavarma.blogspot.com/2021/05/a-52-year-old-male-with-cerebellar.html?m=1
1) What is the evolution of the symptomology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patients problem?
ANS. Timeline of the patient is as follows-
Patient was Diagnosed to Have DeNovo Hypertension in the Past But he did Not take any Medication.
7 days back- Patient gave a history of giddiness that started around 7 in the morning; subsided upon taking rest; associated with one episode of vomiting
4 days back- Patient consumed alcohol; He developed giddiness that was sudden onset, continuous and gradually progressive. It increased on standing and while walking.
H/O postural instability
Associated with bilateral hearing loss, aural fullness, presence of tinnitus
Associated vomiting- 2-3 episodes per day, non projectile, non bilious.
Present day of admission- Slurring of speech, deviation of mouth that got resolved the same day
Anatomical location- There is a presence of an infarct in the inferior cerebellar hemisphere of the brain.
Etiology-
Patient has hypertension for which he has been prescribed medication but he has not taken.There may be an Episode of Stroke which can be due to Ischemic or Heamorhagic cause resulting in reduced blood supply to the Cerebellar region resulting in Infarction.
2) What are the mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
ANS.
1) Tab Vertin - anti- vertigo medication
It is a weak agonist on H1 receptors located on blood vessels of the inner ear. This leads to local vasodilation and increased vessel permeability. This can reverse the underlying problem.
It is used due to patients history of giddiness and balance issues.
2) Tab Zofer 4mg- This is ondanseteron- It is an anti emetic
It is a 5H3 receptor antagonist on vagal afferents in the gut and they block receptors even in the CTZ and solitary tract nucleus.
IUsed to control the episodes of vomiting and nausea in this patient.
3) Tab Atorvostatin 40mg- This is a statin
It is an HMG CoA reductase inhibitor.It decreases blood LDL and VLDL, decreases cholesterol synthesis, thus increasing LDL receptors in liver and increasing LDL uptake and degeneration. Hence plasma LDL level decreases.
Indications- It is used for prevention of stroke.

4) Clopidogrel 75mg- It is an antiplatelet medication
MOA- It inhibits ADP mediated platelet aggregation by blocking P2Y12 receptor on the platelets.
Indications- It decreases the risk of heart disease and stroke by preventing clotting

5) Thiamine- It is vitamin B1
It is naturally found in many foods in the human diet. As the patient is chronic alcoholic thiamine is given prophylactically as there is decreased absorption of nutrients in chronic alcoholics.So that Wenickes Encephalopathy can be prevented.
6) Tab MVT- Multivitamin Tablet
3) Did the patients history of denovo hypertension contribute to his current condition?
ANS. High blood pressure (especially if left untreated) can be a major risk factor for the formation of cerebellar infarcts.
There may Be Endothelial Dysfunction due to high Blood Pressure resulting in abnormality of the blood flow and Formation of Blood Clots leading to stroke.
4) Does the patients history of alcoholism make him more susceptible to ischaemic or haemorrhagic stroke?
Ans) Ischaemic stroke- this is more common. This Is caused by a blood clot blocking the flow of blood and preventing oxygen from reaching the brain
Haemorrhagic stroke- occurs when an aneurysm bursts or when a weakened blood vessel leaks, thus causing cerebral haemorrhage
The adverse effect on BP that is seen due to increased drinking is a major stroke risk factor and increase the risk of heart stroke.
Heavy alcohol intake is associated with impaired fibrinolysis, increased platelet activation and increased BP and heart rate.
So Alcoholism And Hypertension may be the Cause of his Condition.
NEUROLOGY 2(A)
https://143vibhahegde.blogspot.com/2021/05/wernickes-encephalopathy.html
Q)What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans) Patient was Diagnosed with Diabetes Mellitus 2 years ago.
- He developed an episode of seizures 1year back and another episode of seizures 4 months Back(following cessation of alcohol )
- 9 Days Back he started talking to himself and laughing.There was also decreased food intake from then.
- He was unable to lift himself from the bed and move around.He also had short term memory loss
Anatomical localisation
Central Nervous System
Primary Etiology of Patient Problem
Deficiency of Thiamine and Increased levels of toxins in the Body due to Chronic Alcoholism is the Primary Etiology of the Problem in the Patient.
Q) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient ??
Thiamine - it is administered to replenish the depleted stores of thiamine in the body. It also sets back the altered carbohydrate metabolism.
Lactulose - It is given to treat the Uremic Encephalopathy.It Decreases the Ammonia Production in the Body.
Lorazepam - It enhances the inhibitor effects of GABA.
Potchlor - It is used to treat the Low Levels of Potassium.
Daily Dressing of the ulcer.
Q) Why have neurological symptoms appeared this time, that were absent during withdrawal earlier ? What could be a possible cause for this ??
May be due to excess thiamine Deficiency and excess toxin accumulation.
Q) What is the reason for giving thiamine in this patient ??
In chronic alcoholic patients there will be inadequate nutritional intake and also decreased absorption of thiamine from gastrointestinal tract.
There will also be impaired utilisation of thiamine in cells.
There are some enzymes participating in carbohydrate metabolism like pyruvate dehydrogenase and transketolase which are are mainly dependent on thiamine for their function. But as there is thiamine deficiency in chronic alcoholics the carbohydrate metabolism will be altered.
Altered carbohydrate metabolism main lead to oxidative stress resulting in excess of highly reactive free radicals and decreased
Cerebellum particularly the Vermis is also so sensitive to Thiamine Deficiency, which indirectly affect neurocognitive functions attributable to frontal lobe by disrupting the the neural pathways connecting 2 brain regions.
So Thiamine is given in this patient to compensate the deficiency.

Q ) What is the the probable cause of kidney injury in this patient ??
Maybe the decreased fluid intake from past 9 days resulted in in decreased glomerular perfusion causing Pre Renal Acute Kidney Injury.
Q) What is the probable cause of normocytic anaemia in this patient??
As the kidney is injured maybe the erythropoietin deficiency is the cause of anaemia in this patient.
NEUROLOGY (G)
https://amishajaiswal03eloggm.blogspot.com/2021/05/a-50-year-old-patient-with-cervical.html
Q) What is myelopathy hand ??
Loss of power of adduction and extension of the ulnar two or three fingers and an inability to grip and rapidly release with these fingers is termed as myelopathy hand. This is due to Pyramidal Tract Involvement.

Q) What is finger escape ??
It is a neurological sign consisting of involuntary abduction of the fifth finger due to unopposed action of the the extensor digiti minimi. This is seen in cervical myelopathy.
Q) What is Hoffmans Reflex ??
It is a test used to examine the reflexes of upper extremities.
It tests for the possible existence of spinal cord compression.
NEUROLOGY (D)
https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
Q) Is there any relationship between occurrence of seizure to brain stroke. If yes what is the mechanism behind it?
Seizures after haemorrhagic strokes are thought to be attributable to irritation caused by products of blood metabolism. The exact pathophysiology is unclear, but an associated ischaemic area secondary to haemorrhage is thought to play a part. Late onset seizures are associated with the persistent changes in neuronal excitability and gliotic scarring is most probably the underlying cause.
NEUROLOGY (F)
http://shivanireddymedicalcasediscussion.blogspot.com/2021/05/a-30-yr-old-male-patient-with-weakness.html
Q) 1.Does the patient's history of road traffic accident have any role in his present condition?
A:One cause of stroke after trauma is a tear in the head or neck blood vessels that lead to the brain, which can be a source of blood clots that cause a stroke. If a tear in these arteries can be diagnosed at the time of the trauma, a patient could be treated with an anti-clotting medicine to help prevent stroke
2.What are warning signs of CVA??
- Sudden NUMBNESS or weakness of face, arm, or leg, especially on one side of the body.
- Sudden CONFUSION, trouble speaking or understanding speech.
- Sudden TROUBLE SEEING in one or both eyes.
- Sudden TROUBLE WALKING, dizziness, loss of balance or coordination.
- Sudden SEVERE HEADACHE with no known cause.
3) What is the Drug rationale in CVA??
Aspirin - Anti Platelet

Atorvastatin - Decreases the level of Plasma LDL

Clopidogrel

4. Does alcohol has any role in his attack?
Heavy alcohol consumption has been associated with an increased risk of stroke and stroke mortality. In addition to alcohol consumption, the most important risk factors for stroke are hypertension, coronary artery disease, cardiac insufficiency, atrial fibrillation, type 2 diabetes, smoking, overweight, asymptomatic carotid artery stenosis and elevated levels of cholesterol.
5.Does his lipid profile has any role for his attack??
Yes increased LDL causes atherosclerosis which ultimately results in stroke.
NEUROLOGY (C)
http://bejugamomnivasguptha.blogspot.com/2021/05/a-45-years-old-female-patient-with.html
1Q)What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem ??
Ans.
Evolution of Symptoms :
Patient was normal 8 months back then developed b/l pedal edema which was gradually progresive.
Palpitations :since 5days, sudden in onset which is more during night
Dyspnoea during palpitations (NYHA-3) since 5 days
Pain:since 6days, radiating along left upper limb.
Chest pain since 5 days.
Anatomical localisation :
Palpitations can be localised to CVS.
Dyspnea can be localised to CVS
Respiratory System
Pedal Edema can be localised to CVS,Liver,Renal Systems.
Chest Pain can be localised to CVS.
Etiological Agent :
May be Hypokalemia is Causing Palpitations.
Radiating Pain Along Upper Limb is due to Cervical Spondylosis.
2Q) What are the reasons for recurrence of hypokalemia in her? Important risk factors for her hypokalemia?
Important Risk factors for Hypokalemia :
1)Medications-diuretics, laxatives, enema.
2)alkalosis, 3)thyrotoxicosis,
4)anorexia, 5)dementia
3) What are the changes seen in ECG in case of hypokalemia and associated symptoms?
A) changes seen in ECG :
Earliest change :decreased T-wave amplitude, ST depression, Twave - and inversion or flat;prolonged PR interval;presence of Uwaves
In Severe cases :ventricular fibrillation.

Symptoms of hypokalemia :
Weakness & fatigue, palpitations, muscle cramps , anxiety, psychosis.
NEUROLOGY (E)
https://nikhilasampathkumar.blogspot.com/2021/05/a-48-year-old-male-with-seizures-and.html?m=1
Q1) What could have been the reason for this patient to develop ataxia in the past 1 year ??
There is history of Multiple Falls and Minor Head Injuries.And He is even Addicted to Alcohol from Past 3 years.
May be these 2 reasons combinely has caused Ataxia.
Q2)What was the reason for his IC bleed? Does Alcoholism contribute to bleeding diatheses ?
High Alcohol Consumption Leads to Intra Cerebral Heamorhage.Alcoholics are prone to Subdural Hematoma as a consequence of Head Injury in intoxicated State.
NEUROLOGY (H)
https://neerajareddysingur.blogspot.com/2021/05/general-medicine-case-discussion.html?m=1
1) What can be the cause of her condition ?
Presence of Cortical Vein Thrombosis in Right Posterior Temporal Lobe.
2 ) What are the risk factors for cortical vein thrombosis?
Iron Deficiency Anemia
Hereditary Thrombophilia
Trauma
Sickle Cell Anemia
4) What drug was used in suspicion of cortical venous sinus thrombosis ??
Clexane - Enoxaparin was used in Suspicion of Cortical Venous Sinus Thrombosis
3)CARDIOLOGY(D)
https://daddalavineeshachowdary.blogspot.com/2021/05/67-year-old-patient-with-acute-coronary.html?m=1
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
TIMELINE OF EVENTS-
• Diabetes since 12 years - on medication
• Heart burn like episodes since an year- relieved without medication
• Diagnosed with pulmonary TB 7 months ago- completed full course of treatment, presently sputum negative.
• Hypertension since 6 months - on medication
• Patient presented with Shortness of Breath
Anatomical localisation - Cardiovascular system
Etiology: The patient is both Hypertensive and diabetic and these may result in the development of atherosclerosis.
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Pharmacological interventions:
TAB MET XL 25 MG/STAT-contains Metoprolol as active ingredient
MOA: METOPROLOL is a cardiselective beta blocker
Beta blockers work by blocking the effects of the hormone epinephrine. Beta blockers have a negative chronotropic effect
and negative inotropic effect.
Beta blockers also have antiarrhythmic effects and also anti ischemic effects. They also inhibit renin.
EFFICACY STUDIES.
In CAD, 12 meta-analyses (93 RCTs, 103,481 patients) showed that beta-blockers reduced mortality in analyses before routine reperfusion, but there was a lack of benefit in contemporary studies where ≥ 50% of patients received thrombolytics or intervention.
Non pharmacological intervention advised to this patient is: PERCUTANEOUS CORONARY INTERVENTION.
Percutaneous Coronary Intervention is a non-surgical procedure that uses a catheter (a thin flexible tube) to place a small structure called a stent to open up blood vessels in the heart that have been narrowed by plaque buildup ( atherosclerosis).

3) What are the indications and contraindications for PCI?
INDICATIONS:

CONTRAINDICATIONS:
Absence of cardiac surgery backup.
Hypercoagulable state.
High-grade chronic kidney disease.
Chronic total occlusion of SVG.
4) What happens if a PCI is performed in a patient who does not need it? What are the harms of overtreatment and why is research on overtesting and overtreatment important to current healthcare systems?
Although PCI is generally a safe procedure , it might cause serious certain complications like
A)Bleeding
B) Blood vessel damage
C) Allergic reaction to the contrast dye used
D) Arrhythmias
E) Need for emergency coronary artery bypass grafting .
⁃ OVER TESTING AND OVER TREATMENT :
In olden days doctors would so much depend on their intuition as technology was not available .But these days every physician is dependent on laboratory reports.We cannot say it is a bad thing as it would lead to accurate diagnosis, but the point is these should be used logically only where they are required.Or else it would lead to overtesting.And overtesting has its own adverse effects.For example during the recent 2nd wave of Covid Pandemic majority of the Covid Patients including the asymptomatic and patients with mild disease were advised to take CT Scan which lead to unwanted radiation exposure.Even overtreatment has its own adverse effects.So even though all the Therapeutic and Diagnostic Facilities are available at our disposal , Physicians should use them Judiciously or Else they will do more harm than good.
3) CARDIOLOGY (B)
https://muskaangoyal.blogspot.com/2021/05/a-73-year-old-male-patient-with-pedal.html
QUESTION: What are the possible causes for heart failure in this patient ??
1. Chronic Uncontrolled Diabetes
2. Chronic Alcoholism
3. Anemia Due to CKD may lead to Left Ventricular Hypertophy and Diastolic Dysfunction then Finally resulting in Heart Failure.
QUESTION: what is the reason for anaemia in this case ??
Anemia in this Patient is may be due to Chronic Kidney Disease. Erythropoietin is required for the Production of RBC in erythropoiesis.
Erythropoietin (EPO) is produced mainly from Peritubular Interstitial Fibroblasts of the Kidney .As Tubular interstitium is involved in CKD ,EPO production will be reduced.This results in decreased production of RBC leading to Anemia.
There is Also a Possibility of Anemia of Chronic Diseases.

QUESTION: What is the reason for blebs and non healing ulcer in the legs of the patient ??
May be Uncontrolled Diabetes Mellitus may be the cause for non Healing ulcer.

QUESTION: What sequence of stages of diabetes has been noted in this patient ??
Initially Patient was diagnosed with Diabetic Mellitus.Then patient Developed Diabetic Retinopathy And Diabetic Nephropathy leading to Chronic Kidney Disease.
3) CARDIOLOGY (A)
https://muskaangoyal.blogspot.com/2021/05/a-78year-old-male-with-shortness-of.html
1.What is the difference btw heart failure with preserved ejection fraction and with reduced ejection fraction?
In Heart Failure with Preserved Ejection Fraction (HFPEF) there is increased Right Ventricular Filling Pressure resulting in Ascitis,Edema,Hepatomegaly. Causes of HFPEF :
1) Systolic Hypertension. 2) Restrictive Cardiomyopathy. 3) Chronic Constructive Pericarditis. 4)Hypertrophic Cardiomyopathy
In HF with Reduced Ejection Fraction(HFREF) there will be increased Left Ventricular Pressure causing Pulmonary Congestion;and there will also be Decreased Stroke volume leading to Fatigue,Dyspnea,narrow Pulse Pressure.
2.Why haven't we done pericardiocenetis in this pateint?
As far As I know Pericardiocentesis is Useful mainly in Cardiac Tamponade to drain the Blood Accumulated in the Pericardium.But This Patient isn't having Cardiac Tamponade.So Pericardiocentesis is Not Required.
May Be Pericardial Biopsy Can Be Done.
3.What are the risk factors for development of heart failure in the patient?
May Be Anemia is the Reason for the Development of Heart Failure In This Patient. Alcohol And Smoking have additive effects.
4.What could be the cause for hypotension in this patient?
May be Pericardial effusion Has lead to Decreased Cardiac Output .And Decreased Cardiac Output May Result in Hypotension.
CARDIOLOGY (C)
https://preityarlagadda.blogspot.com/2021/05/biatrial-thrombus-in-52yr-old-male.html
1Q)What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans. Shortness of Breath - From 2 DAYS.
Decreased Urine Output-From 2 Days
Anatomical Localization : Heart
Etiology : Atrial Fibrillation
2Q) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans. Inj.Dobutamine -Ionotropic Action so Increase the force of. Contraction
Tab.Digoxin - Ionotropic Effect
Diuretics Are also used
Beta Blockers is also used.
3Q) What is the pathogenesis of renal involvement due to heart failure (cardio renal syndrome)? Which type of cardio renal syndrome is this patient?
Cardiorenal syndromes (CRS) describe concomitant bidirectional dysfunction of the heart and kidneys in which 1 organ initiates, perpetuates, and/or accelerates decline of the other. CRS are common in heart failure.

4Q )What are the risk factors for atherosclerosis in this patient?
Hypertension
Alcohol
5) Why was the patient asked to get those APTT, INR tests for review?
To Monitor the Risk of Bleeding.
CARDIOLOGY (E)
https://bhavaniv.blogspot.com/2021/05/case-discussion-on-myocardial-infarction.html?m=1
1Q) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Evolution of symptomatology:
Uncontrolled DM2 since 8 years
3 days back Mild chest pain dragging type and retrosternal pain(radiated)
Anatomical localisation: Inferior wall of heart
Primary etiology: Diabetes type 2 (uncontrolled)
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Aspirin - Inhibits Prostaglandins
Atorvastatin - Inhibits HMG Co A reductase there by reduces the Cholesterol Production in the Liver.
Clopodogrel -Inhibits Platelet Aggregation
3Q) Did the secondary PTCA do any good to the patient or was it unnecessary?
Yes the Patient improved after the secondary PTCA and the patient was discharged from the Secondary Centre.It clears the Obstruction and restores the Blood Supply.
CARDIOLOGY (F)
https://kattekolasathwik.blogspot.com/2021/05/a-case-of-cardiogenic-shock.h
1Q) How did the patient get relieved from his shortness of breath after i.v fluids administration by rural medical practitioner?
May be the Shortness of Breath was Due to Decreased Cardiac Output.And as The Rural medical Practitioner has given i.v.fluids the Cardiac Output has increased and Shortness of Breath was relieved.
2. What is the rationale of using torsemide in this patient?
Torsemide is used to increase the urine output
3. Was the rationale for administration of ceftriaxone? Was it prophylactic or for the treatment of UTI?
There was whitish discharge in the Urine.Hence patient was given Ceftriaxone to treat UTI.
4th Question (C) GASTROENTEROLOGY
https://chennabhavana.blogspot.com/2021/05/general-medicine-case-discussion-1.html
1) what is the most probable diagnosis ??
Ruptured liver abscess may be the most probable diagnosis
2) What was the cause of her death?
As we can see from his liver function test and renal function test that there is abnormal increase in alkaline phosphatase and also in the urea and creatinine so there may be a chance that impaired liver and renal functioning may be the reason for his death. As laparotomy was done on the patient the day before his death may be any complication of the procedure may also be the cause of death like hemorrhage and damage to internal organs.
3) Does her NSAID abuse have something to do with her condition? How?
NSAID inhibit the synthesis of prostaglandins. prostaglandins are required for the direction of the afferent arteriole of the kidney. But as their synthesis is inhibited there will be no afferent arteriolar dilation and reduced glomerular perfusion this may lead to pre renal acute kidney injury.Chronic NSAIDs use has also been related to hepatotoxicity. While the other adverse effects of NSAIDs such as are well known, gastrointestinal mucosal injury NSAIDs have also been associated with hepatic side effects ranging from asymptomatic elevations in serum aminotransferase levels and hepatitis with jaundice to fulminant liver failure and death.

GASTROENTEROLOGY (B)
https://nehae-logs.blogspot.com/2021/05/case-discussion-on-25-year-old-male.html
1) What is causing the patient's dyspnea? How is it related to pancreatitis?
May be Pancreatitis is the Cause of Patients Dyspnea.Once Pancreatitis is initiated the inflammatory events within the acinar cells will progress to a generalized systemic inflammatory response syndrome (SIRS). Amongst the systemic complications, pulmonary complications are the most frequent and potentially the most serious.
The most dangerous complication of the pulmonary system is ARDS.
Activated trypsin causes damage to pulmonary vasculature and increases endothelial permeability. Active circulating phospholipase A2 (PLA2) is known to remove fatty acids from phospholipids. One of the main components of surfactant is the phospholipid, dipalmitoylphosphatidylcholine. Many recent studies have assessed the role of platelet activating factor (PAF) which stimulates polymorphonuclear cells (PMNs) regulating the interaction between PMNs and endothelial cells facilitating migration of activated WBC into interstitial spaces.
There are pro-inflammatory cytokines released from the pancreas such as tumor necrosis factor-alpha (TNF-α), interleukin (IL)-1, IL-6, and IL-8. PMNs also contribute to release of cytokines
4) What is the line of treatment in this patient?
iv fluids and colloids
NPO (Nill Per Oral)
Analgesics
Nasogastric suction -to decrease gastrin release from stomach
laparotomy and debridement of hemorrhagic pancreatic tissue.
antibiotic therapy like ciprofloxacin , ofloxacin, imipenem
5 (A) Nephrology
https://kavyasamudrala.blogspot.com/2021/05/medicine-case-discussion-this-is-online.html
1) What could be the reason for SOB??
As the patient was administered diuretics may be it has lead to increased excretion of Bicarbonate ions.So there will be Metabolic Acidosis.To compensate that there will be increase in the respiratory rate to eliminate the CO2 so that equilibrium is maintained.Hence there will be Shortness of Breath due to increased respiratory rate.
2) Why does he have intermittent episodes of drowsiness??
Use of Diuretics has lead to Hyponatremia which resulted in Drowsiness.
3)Why did he complain of fleshy mass like passage in urine ??
There are large no. Of puss cells in his urine.May be the patient confused these with a fleshy Mass.
4)What are the complications of TURP that he may have had ??
TURP -Transurethral resection of Prostate
- May be Glycerol used for bladder wash during the procedure has caused some damage to the kidney.There was a rise in his creatinine levels following the procedure.
There is also chance of infection.
Patient's WBC count is also Raised.

NEPHROLOGY (B)
https://drsaranyaroshni.blogspot.com/2021/05/an-eight-year-old-with-frequent.html
1Q) Why is the child excessively hyperactive without much of social etiquettes ?
May Be the Child is Suffering from ADHD
(Attention Deficit Hyperactivity Disorder).
Mechanism of ADHD :

2Q) Why doesn't the child have the excessive urge of urination at night time ? ?
May be the excessive urination of the child is a Psychological Problem (Related to ADHD).So there is Excessive Urination only when the Patient is Awake.
3Q) How would you want to manage the patient to relieve him of his symptoms ??
Amphetamine which is a CNS stimulant will be useful in this Patient.
I would also try to change the Parenting Behaviour and teach the parents Positive Reinforcement Methods so that the child would get A Good Family Support.
Cognitive Training should also be Given to the child.
6) INFECTIOUS DISEASE
A) https://vyshnavikonakalla.blogspot.com/2021/05/a-40-year-old-lady-with-dysphagia-fever.html
Q) 1.Which clinical history and physical findings are characteristic of tracheo esophageal fistula?
Laryngeal Crepitus,Difficulty in swallowing initially to the solids,
Cough,are Suggestive of TracheoEsophageal Fistula.
Q) What are the chances of this patient developing immune reconstitution inflammatory syndrome? Can we prevent it?
Risk Factors For Development of Immune Reconstitution Inflammatory Syndrome (IRIS)
1) Low Baseline CD4 Count
2) Higher Baseline Viral Load
3) Shorter Interval between commencing ATT and HAART
4) Disseminated TB
5) A Greater Decrease in Viral Load after starting HAART.
As this patient has a low baseline CD4 count and also disseminated TB there are chances that this patient may develop IRIS.

If the following symptoms are seen after the Initiation of ART then IRIS can be suspected
1) Fever,Anemia,Wt loss.
2) CNS
3) Lymphadenopathy
4) Radiological Findings
5) Exacerbation of Pulm. Lesion or occurence Of a new Lesion.
Prevention of IRIS :
CD4+ T cell deficiency when ART is commenced is a risk factor for an IRIS, prevention of CD4+ T cell depletion through early diagnosis and treatment of HIV infection regardless of CD4+ T cell count, as supported by the findings of the START study (33), is the most effective measure for reducing the risk of developing an IRIS.
However, 'late presenters' with advanced immunodeficiency continue to present and they must be assessed carefully for HIV-related infections that might trigger an IRIS when ART is commenced.
7th Question (B)
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-liver-abcess.html
1) Cause of liver Abcess in this Patient??
May be due to malnutrition and lack of personal hygeine is the cause of the infection in the patient resulting in liver abcess. The infection may be amoebic or any other bacterial infection.
2) How do you approach this Patient??
As the patient presented with the pain in the abdomen, first I would go for a USG abdomen and As USG showing hyperechoic mass on the liver I would also do LFT(Liverfunction Test)
As there is a mass as seen in USG and LFT is also abnormal (Raised ALP), I would start empirical Treatment for both Amoebic and pyogenic liver abscess.
According to the response given to this Medical Treatment it will be decided whether aspiration is required or not.

3) why do we treat both amoebic and pyogenic liver abscess ??
Even though amoebic liver abscess is confirmed as a diagnosis there is a chance of super infection with bacterial organisms so there is a need for treating both amoebic liver abscess and pyogenic liver abscess
4) Is there a way to confirm definitely diagnosis in this patient ??
Amoebic liver abscess can be confirmed by serology for entamoeba.
7 (A) Infectious Disease and Hepatology
https://kavyasamudrala.blogspot.com/2021/05/liver-abscess.html
Liver abscess
1Q) Do you think drinking locally made alcohol caused liver abscess in this patient due to predisposing factors present in it ??
Yes, may be the liver Abcess developed due to the chronic intake of contminated Toddy.
2) What is the etiopathogenesis of liver abscess in a chronic alcoholic patient ? ( since 30 years - 1 bottle per day)
Chronic alcohol intake especially the locally available contaminated drinks plays a major role in the formation of liver abscesses which can be either Amoebic or Pyogenic liver abscess because of the adverse effects of alcohol over the Liver.
3) Is Liver Abcess more common in Right Lobe ??
50% of solitary liver abscesses occur in the right lobe of the liver (a more significant part with more blood supply), less commonly in the left liver lobe or caudate lobe.
4) what are the indications of Ultrasound-guided aspiration of Liver abscess ??
Indications for USG guided aspiration of liver abscess
1. Large abscess more than 6cms
2. Left lobe abscess
3.Caudate lobe abscess
4. Abscess which is not responding to drugs
8) INFECTIOUS DISEASE (Mucormycosis)
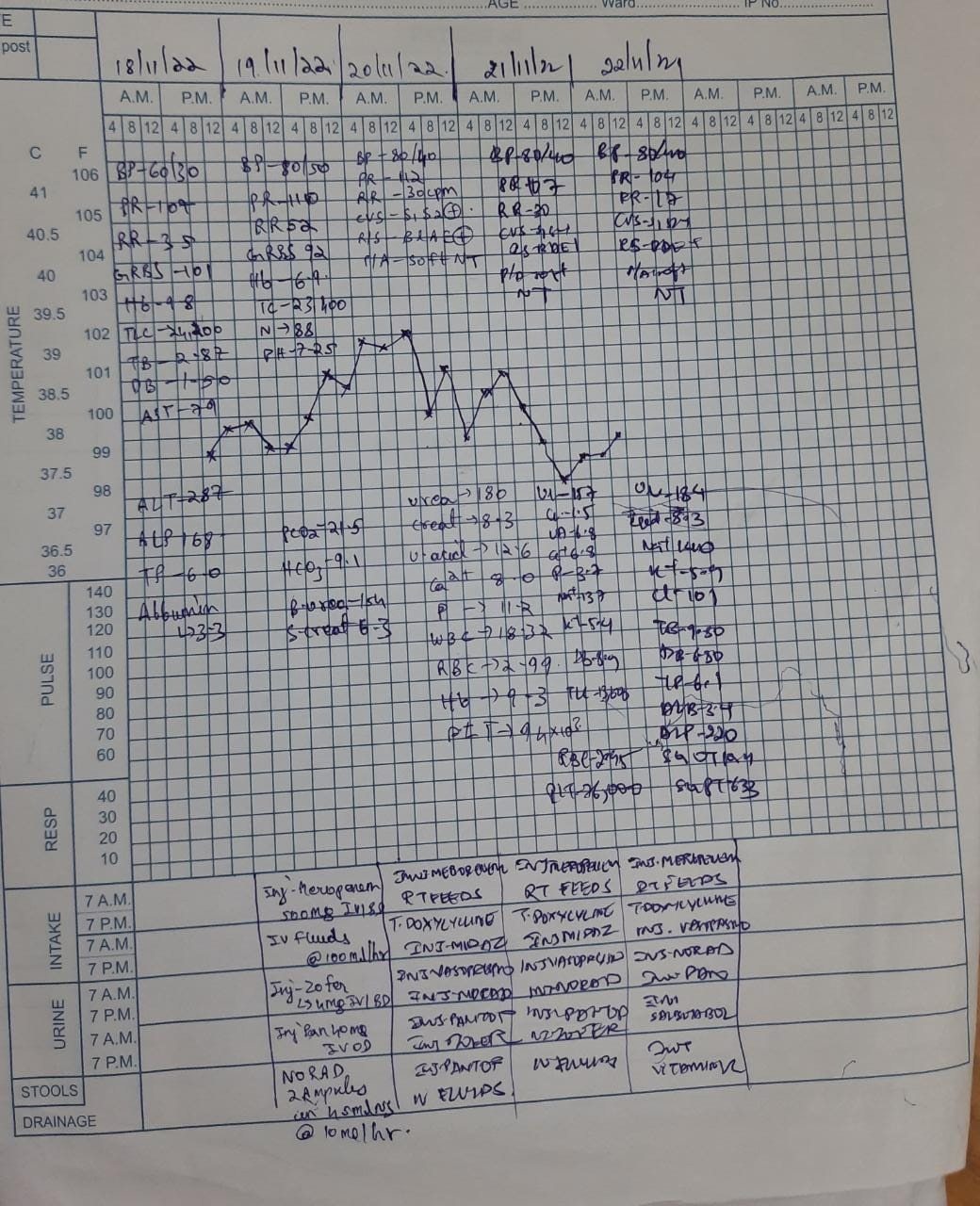
http://manikaraovinay.blogspot.com/2021/05/50male-came-in-altered-sensorium.html
1) QUESTION: What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary aetiology of the patient's problem?
1. 3 years ago diagnosed with hypertension
2. 21 days ago he received vaccination at local PHC which was followed by fever associated with chills and rigors, high grade fever.
3. 18 days ago he complained of similar events and went to the the local hospital, it was not subsided upon taking medication.
4. 11 days ago he complained of Generalized weakness and facial puffiness and periorbital oedema. Patient was in a drowsy state
5. 4 days ago-
a. patient presented to casualty in altered state with facial puffiness and periorbital oedema and weakness of right upper limb and lower limb
b. towards the evening patient periorbital oedema progressed
c. serous discharge from the left eye that was blood tinged
d. was diagnosed with diabetes mellitus
6. patient was referred to a government general hospital
7. patient died 2 days ago
Patient wasn't aware of his diabetic condition until then. He was also suffering from diabetic acidosis.This resulted in poorly controlled blood sugar levels. The patient was diagnosed with acute rhinocerebral mucormycosis. Rhino cerebral mucormycosis is the most common form of this fungal disease that occurs in people with uncontrolled diabetes.The fungus enters the sinuses from the environment and then the brain.
The patient was also diagnosed with acute infarct in the left frontal and temporal lobe. Mucormycosis is associated with the occurrence of CVA
2) QUESTION: What is the efficacy of drugs used along with other non-pharmacological treatment modalities and how would you approach this patient as a treating physician?
The proposed management of the patient was –
1. inj. Liposomal amphotericin B according to creatinine clearance
2. 200mg Iitraconazole was given as it was the only available drug which was adjusted to his creatinine clearance
Management of diabetic ketoacidosis –
a) Fluid replacement- The fluids will replace those lost through excessive urination, as well as help dilute the excess sugar in blood.
(b) Electrolyte replacement-The absence of insulin can lower the level of several electrolytes in blood. Patient will receive electrolytes through a vein to help keep the heart, muscles and nerve cells functioning normally.
(c) Insulin therapy- Insulin reverses the processes that cause diabetic ketoacidosis. In addition to fluids and electrolytes, patient will receive insulin therapy

Granulocyte stimulating factors may also be used in the treatment of mucormycosis.
Hyperbaric oxygen can also be used as an adjunctive therapy.
3) QUESTION: What are the postulated reasons for a sudden apparent rise in the incidence of mucormycosis in India at this point of time?
I think it is because of the use steroids in an uncontrolled manner.
COVID 19 is not the first disease where steroids are used as one of the main stay of treatment (in severe cases) but what has gone wrong in the recent time is even the lay man who got infected with Corona started using steroids right from the day 1 with no monitoring by a specialised physician.And they are not following any specific course of treatment.As many of them are also diabetic patients the are getting succumbed to mucormycosis.And it is not ending with mucormycosis but various other fungii are emerging to cause an epidemic.
And another reason for rise in mucormycosis cases may be the usage of tap water in oxygen concentrators.As most of the patients are being diagnosed of Covid in late stages in the second wave many of them Are requiring oxygen concentrators for supplemental oxygenation.And due to Lack of the people are using tap water instead of distilled water which serves as reservoir for the growth of mucormycosis.So this may be one of the reason for rise in mucormycosis cases.


Comments
Post a Comment